BIM and laser scanning in hospital operations: Digital as-built surveys as the key to safe refurbishment
by Kai Weist & Sarah Zonsius | May 26th, 2026
Hospitals are never truly finished; they are constantly being transformed, extended and modernised. And this always takes place under a condition that is not common in conventional construction: whilst the hospital remains in operation. This circumstance makes hospital construction one of the most complex disciplines in building construction and, at the same time, presents a unique opportunity for digital methods. BIM and 3D laser scanning can make a decisive contribution here: as the basis for reliable planning, transparent coordination and efficient digital hospital operations.
Hospital construction: a special case in building construction
Hardly any other type of building combines so many requirements within such a confined space as a hospital. Operating theatres, intensive care units, laboratories, central sterile supply departments and medical technology infrastructure result in an exceptionally high density of building services. Redundant power supplies, medical gases, cleanroom technology and highly specialised ventilation systems are closely interlinked, meaning that coordination conflicts arise not in the architectural design but within the technical framework.
Added to this is structural pressure: the investment backlog in German hospitals is estimated at between 30 and 50 billion euros. With the hospital reform and the transformation fund of over 50 billion euros (2026–2035), the pressure to act is increasing significantly. Refurbishments, extensions and new builds must be completed more quickly than ever before, often whilst the hospital is operating at full capacity.
The Federal Institute for Research on Building, Urban Affairs and Spatial Development (BBSR) has addressed this issue through the KlinikBIM research project: a 169-page guide produced by RWTH Aachen University sets out, for the first time, a robust standard for BIM implementation in hospital construction; this standard defines guidelines ranging from the client’s information requirements (AIA) through to integration into day-to-day operations.
Building whilst operations continue: a particular challenge
What is considered the exception in other sectors is the norm in hospital construction: refurbishment and extension work takes place whilst patients are being cared for in adjacent areas. This places exceptional demands on planning, coordination and execution:
- Noise and dust control must be strictly monitored, as construction dust can increase the risk of infection and compromise hygiene barriers.
- Shutdown periods must be planned precisely: short time slots, often at night or at weekends, require meticulous coordination in advance.
- Logistics within the existing building are complex: transport routes, storage areas and access points must be coordinated with clinical operations.
- Infection control measures (e.g. ICRA – Infection Control Risk Assessment) must be taken into account in every trade.
- Scanning activities and site inspections must be planned in such a way as to ensure patient safety and data security.
Missing or outdated as-built documentation makes all of this even more difficult. If the actual location of an exhaust air duct is unknown or a drainage system is missing from the plans, surprises arise on site which have direct consequences for deadlines, costs and clinical operations.
"In hospital construction, any delay is more than just a financial problem – it can have a direct impact on medical procedures."
Kai Weist
Laser scanning in hospital settings: Digital reality capture without disrupting operations

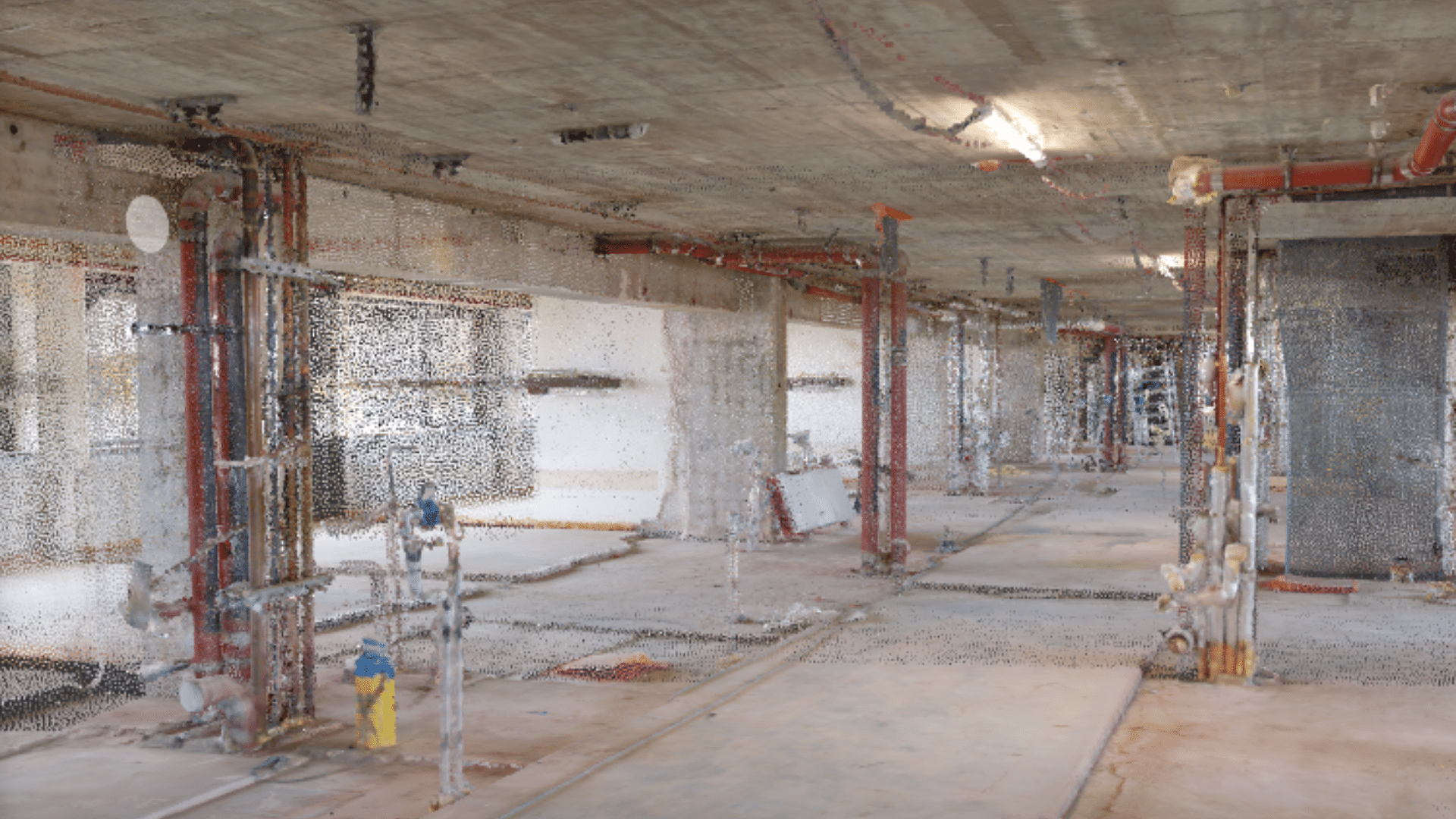
3D laser scanning is a measurement technology in which a rotating laser beam captures millions of measurement points in a very short space of time, generating a highly accurate three-dimensional point cloud of the actual building. This method offers significant advantages in hospital operations:
- Minimal disruption to operations: Scans can be carried out during night shifts or during quieter periods of operation. Modern laser scanners can capture entire corridors and plant rooms in a matter of minutes.
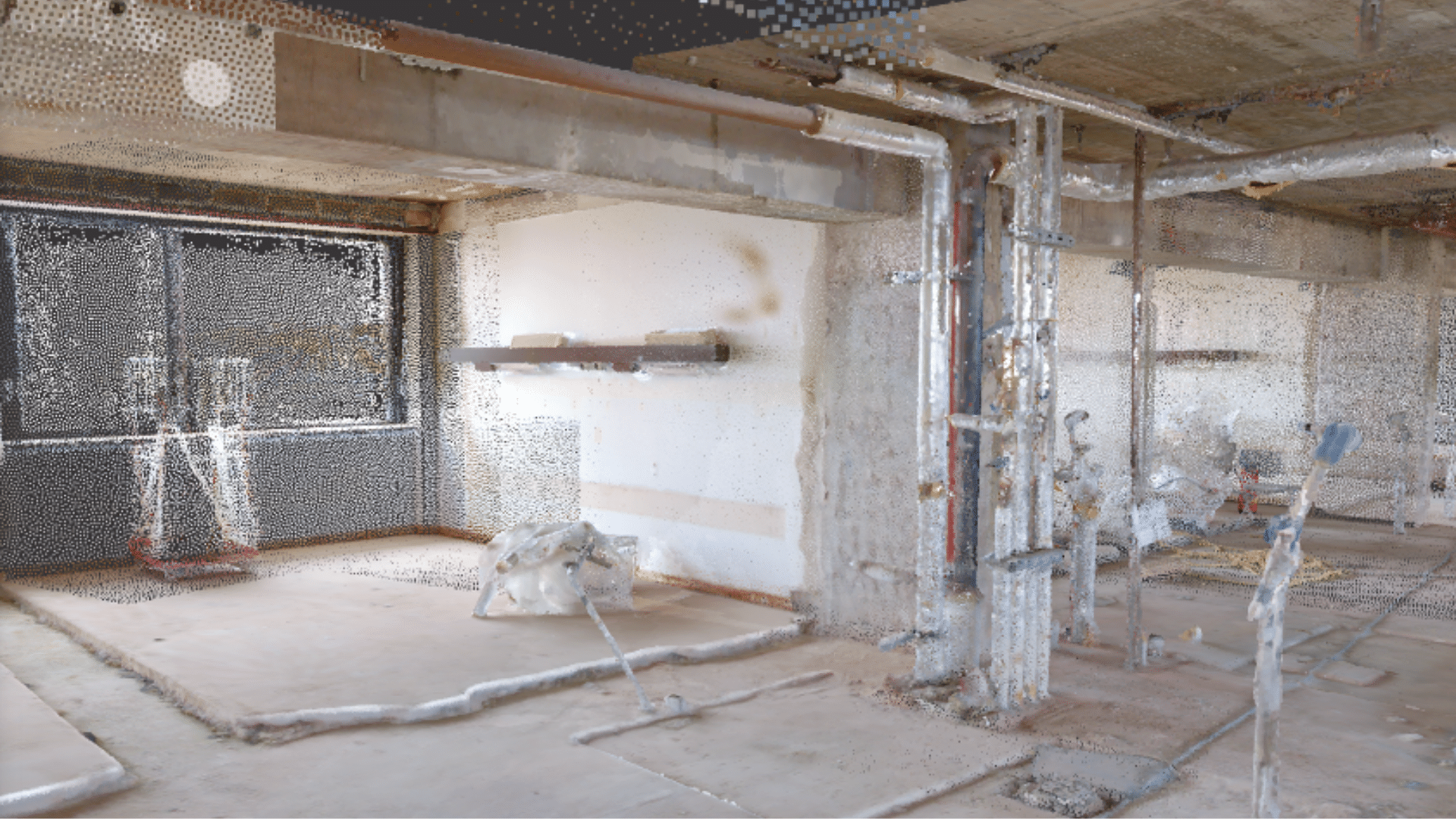
- As-built survey with millimetre accuracy: Hospitals have often undergone refurbishments over decades, which have rarely been fully documented. The laser scan provides the actual current condition, regardless of what is shown on the plans.
- Mapping of complex building services systems: Laser scanning really comes into its own with highly dense technical installations (ventilation, medical gas, IT cabling, fire protection), revealing collisions, spare space and the actual positions of components.
- Data protection-compliant operation: Professional scanning service providers work to clearly defined protocols to ensure that no patient-related data is recorded.
Compared with conventional manual surveys, laser scanning reduces the time and effort required for data collection by up to 60 per cent. For large hospital buildings, which would otherwise take months to survey, this represents a significant economic advantage.
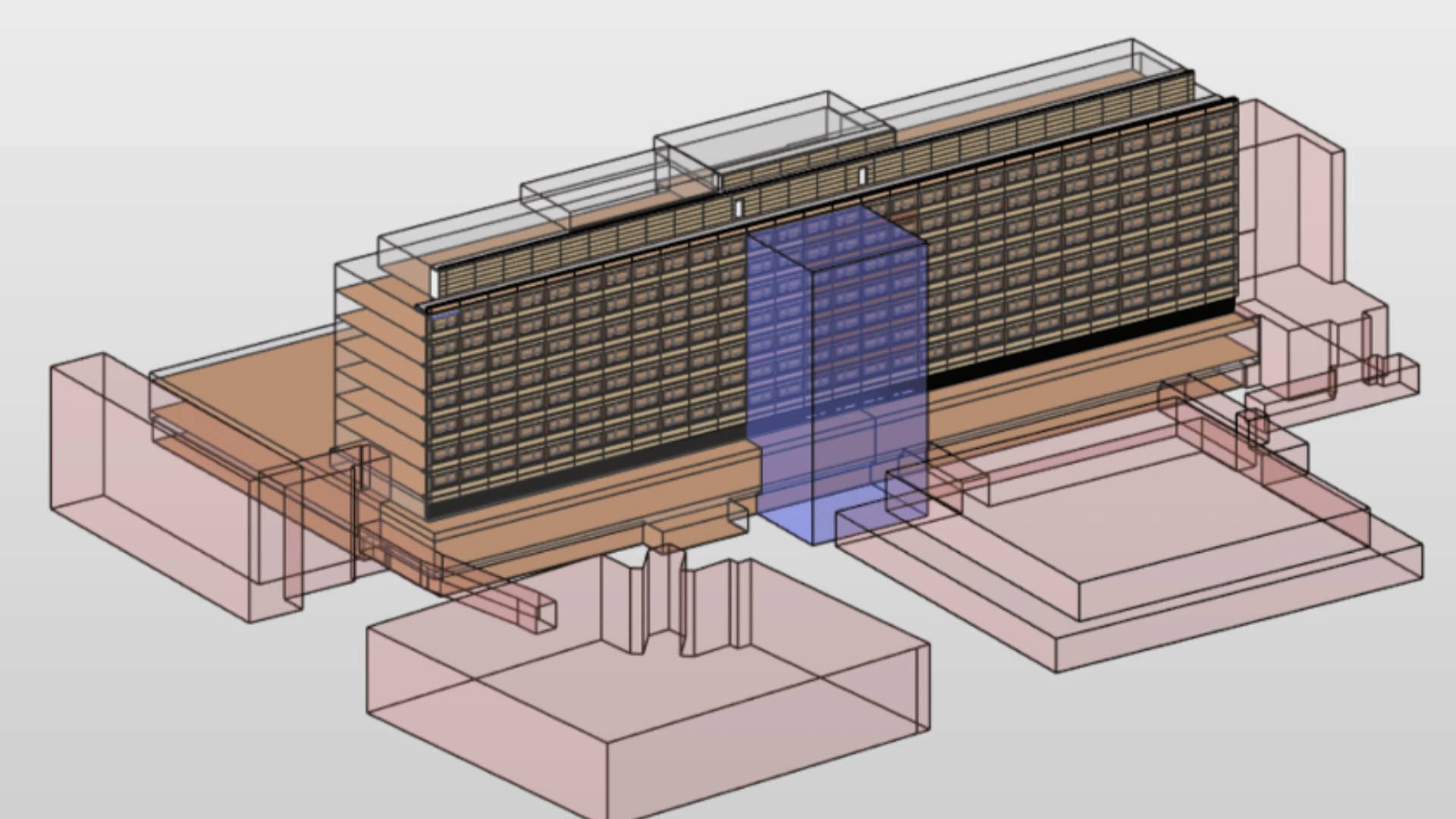
Scan2BIM: From laser scan to structured as-built model
The next step after the as-built survey is modelling: the point cloud is used to create a structured BIM model – the so-called Scan2BIM process. In this process, the point cloud is used as a reference to create a digital information model that combines geometric structure and alphanumeric data.
For hospital construction, a usage-oriented approach is crucial: not every area of a hospital requires the same level of modelling detail. In line with the BIM4FM principle – ‘as much as necessary, as little as possible’ – it is determined which data is actually required for which specific application:
- For refurbishment projects carried out whilst the facility is in operation, precise geometries of the building services systems and the structural framework are essential to identify clashes during the planning stage and avoid costly surprises on site.
- For space and cleaning management, a simplified room structure with room master data, floor area details and component information on surfaces is often sufficient.
- For maintenance and upkeep, the focus is on plant identification, location and links to technical data.
The as-built model produced by the Scan2BIM process is not a blueprint from a new build – but a reliable, validated representation of the building’s actual condition. It forms the basis for all further planning steps in existing buildings.
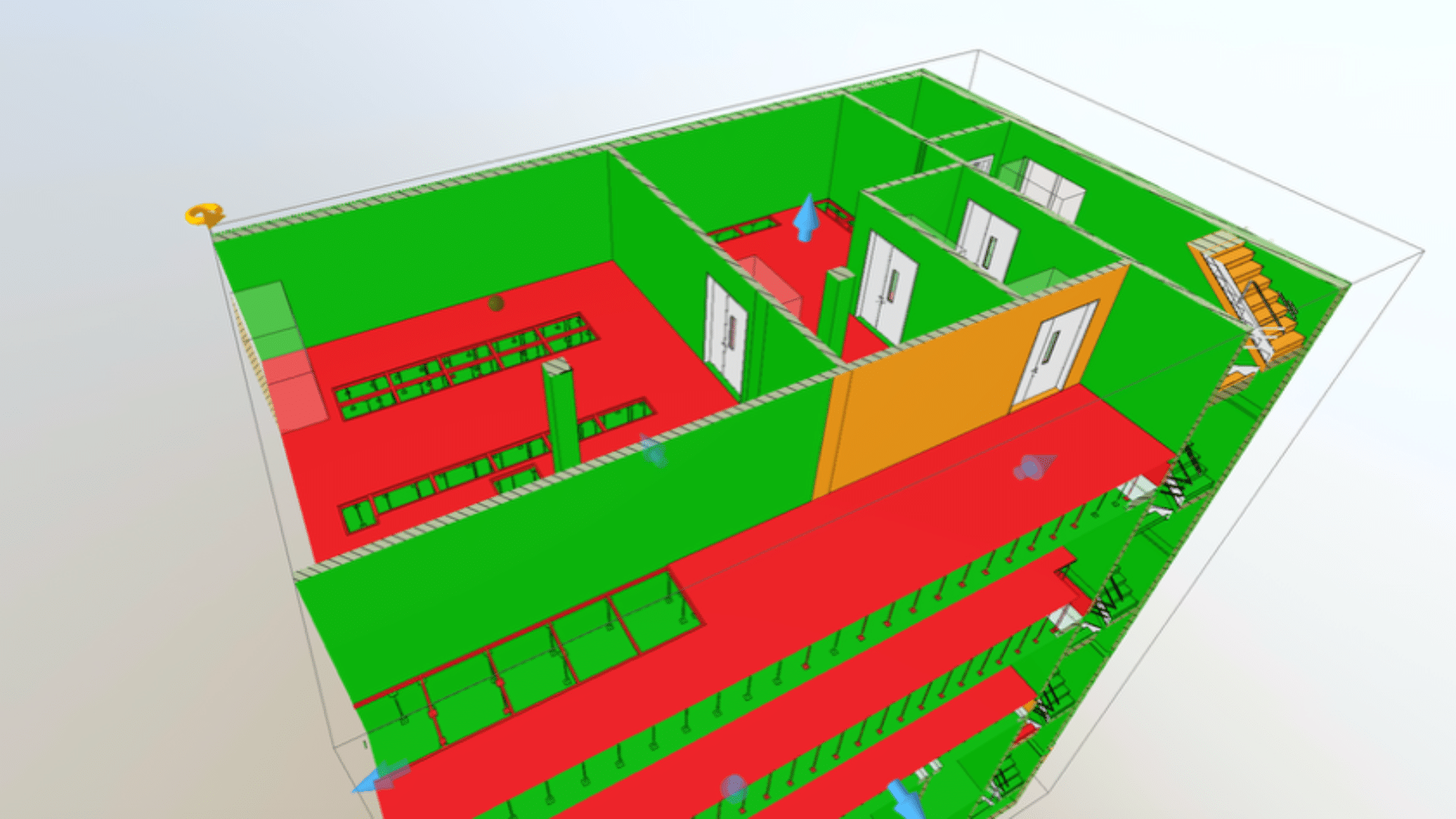
Construction progress monitoring: Automated target-actual comparison with colour-coded visualisation
In hospital construction, seamless monitoring of construction progress is particularly critical, as any delay has a direct impact on day-to-day operations, ward occupancy and patient care. This is precisely where laser scanning offers a further, often underestimated benefit: the automated, AI-supported comparison of the actual state against the target state between the point cloud and the BIM model.
The principle is very straightforward: at regular intervals – weekly or following defined construction phases – the building site is rescanned. Specialised software platforms automatically compare the resulting point cloud with the stored BIM model and the construction schedule. The result is not a subjective status report, but an objective, component-by-component analysis of the actual progress of the works.
- Green – installed correctly: The component has been installed within the defined tolerance and corresponds to the BIM model.
- Orange – installed incorrectly: The component is present but deviates from the design in terms of position, geometry or finish, and requires checking or adjustment.
- Red – missing component: The component is planned in the BIM model but has not yet been installed – a direct indication of a delay in the construction schedule.
This traffic-light system makes the project status immediately clear to everyone involved – from the BIM coordinator to the site management team. Any deviations detected are automatically recorded as issues and can be exported as a BCF file to standard design environments, where they can be assigned and tracked directly. For acceptable deviations, it is also possible to automatically update the BIM model to reflect the actual as-built condition, without the need for someone to spend hours manually remodelling it.
For schedule and cost management, the link to the 4D construction schedule is also crucial: based on the scanned as-built situation, the objective degree of completion can be calculated for each trade and construction phase, including the predicted impact on the remainder of the project.
In hospital construction, this information advantage is particularly valuable:
- If a trade is behind schedule, subsequent trades can be rescheduled in good time before bottlenecks arise on site and disrupt ongoing operations.
- Scan-based progress reports provide tamper-proof, dated evidence of the actual construction status, which is essential for the allocation of funds in hospital projects funded by grants.
- Short construction windows during ongoing operations (at night, at weekends) can be accurately assessed and optimally planned for the next scan cycle.
Practical projects show that scan-based construction progress monitoring enables cost savings of 8–15 per cent, improves adherence to deadlines by up to 25 per cent and reduces rework by up to 40 per cent – figures which represent significant potential for optimisation in the cost-intensive construction of hospitals.
"The automated comparison of actual against target between the point cloud and the BIM model replaces subjective construction progress reports with objective, colour-coded data – and puts the project team back in control."
Kai Weist
Scan2BIM2FM: Bridging the gap to hospital operations

The real added value only emerges when the BIM model from the Scan2BIM process is linked to facility management; this is at the heart of the Scan2BIM2FM approach. In hospital operations, this means that digital asset inventory is not an end in itself, but rather the starting point for a data-driven operational model.
All information streams converge in the CAFM (Computer-Aided Facility Management) system. Room layouts, plant identifiers and component information from the BIM model are linked to dynamic operational data: maintenance cycles, inspection records, lists of medical devices, hygiene plans and energy data. The unambiguous assignment via BIM IDs eliminates the need for duplicate data maintenance.
What this means in practice for day-to-day hospital operations:
Maintenance technicians can locate equipment directly using the model, thereby reducing search times and minimising downtime.
Areas for cleaning tenders are automatically derived from the model without the need for manual measurements.
Relocations and ward occupancy planning can be simulated using the model, which is often a critical factor during ongoing refurbishments.
Energy efficiency and ESG reporting requirements are effectively supported by the structured database.
The point cloud remains available in the system as a visual representation of reality and is thus used for location identification, condition assessment and training of technical staff.
The Transformation Fund for Hospitals and the increasing ESG requirements are creating pressure to establish this digital infrastructure. Hospitals that invest in Scan2BIM2FM today are not only safeguarding their current refurbishment projects; they are also creating the data foundation for permanently efficient and resilient hospital operations.
Conclusion
In hospital operations, BIM and laser scanning are not forward-looking technologies that will be introduced at some point in the future. They are an operational necessity for anyone wishing to run hospitals safely, efficiently and sustainably, because refurbishment whilst the hospital remains in operation is the norm.
The Scan2BIM2FM approach, complemented by rigorous monitoring of construction progress, bridges the gap between the physical reality of the building and the digital operational model. It provides what is so often lacking in hospital construction: a reliable, up-to-date and usable database for planning, coordination, construction and day-to-day operations.
The crucial question is no longer ‘if’, but ‘when’ and ‘how’: Which areas of the hospital will be digitised first? Which use cases generate the quickest return on investment? And what digital infrastructure is required to ensure the data remains usable in the long term?
How digitised is your inventory documentation at present, and where does your greatest potential lie?
If you too would like to optimise your inventory documentation and operational processes using digital methods, please do get in touch. Together, we will develop a digital strategy tailored to your clinic.